| |
المؤلفون / Authors
الملخص / Abstract
الكلمات المفتاحية / Keywords
أقسام الملف
Introduction
Algorithm
Results and Discussion
References
|
| An algorithm for assessing spine distortion during walking |
| |
| |
Anagheem Ibrahim (1) Housam Hasan Bou Issa (1)
Zafar Yuldashiv (1)
Saint-Petersburg Electrotechnical University ETU (LETI)
aibrakhim@etu.ru |
| |
| Abstract |
|
| In recent years, multiple technical means of medical rehabilitation of patients with diseases of the musculoskeletal system have occurred. They are being used, which require developing techniques for monitoring and observing the effectiveness of rehabilitation. Also, according to statistical records, posture conditions detected in most school-age children are associated with a raised risk of developing disorders accompanied by spinal deformation, which influences a high risk of developing spinal deformity during children's growth. This paper demonstrated an algorithm for assessing spine distortion during walking. The proposed algorithm can be used to assess spinal kinematics disorders objectively. |
|
| Keywords: Spinal kinematics, Biomechanics, Detection algorithm, Reflective markers, Moving platform, Spinal deformity, Medical rehabilitation, Medical imaging. |
|
| |
|
| 1.Introduction |
|
| According to current statistics, spinal disorders like Spondylosis, Sciatica, Spinal Infections, Spinal Stenosis, Scoliosis, Spinal Deformities, and Spinal Tumors are observed in most populations, which is considered a promising field of study. Furthermore, attention should be paid to assessing objective and usable signs to notice spine deformity [1]. Distinguishable technologies and methods are currently used, like magnetic resonance imaging, computed tomography, and myelography using radiopaque substances [2]. |
|
| However, these technologies have disadvantages and usage limitations. Screening examinations usually affect public health because they are associated with radiation load on the patients. Biomechanical analysis of parameters of the patient's activity permits us to recognize those violations of the relations of spinal structures [3]. |
|
| Gait velocity would be one of the essential parameters to gain an accurate assessment of alterations in gait, especially if it were considered that pathological people walk slower than healthy ones [4]. |
|
| The used model associated with reflective measuring markers on the patient's back. Changes in the coordinates of reflective markers from frame to frame and the appearance of the dependence of the migration of vertebrae located in the lumbar spine, chest, and diaphragm [5]. |
|
| In the first stage, the patient is walking with at least ten reflective markers attached to it. |
|
| Part of the markers are a reference and are used for navigation of the optical measuring grid, of which two markers are attached to the acromial processes of the left and right shoulder, the third marker is attached to the cervical vertebra (C5), and the fourth marker is attached to the lumbar vertebra (L3). |
|
| At least six markers are measured and attached to the thoracic vertebrae T1-T12 to assess violations of the kinematics of the spine when walking. The selection of the vertebrae of interest for the attachment of measuring markers is carried out based on a preliminary analysis of the X-ray of the vertebral column and the identification of degenerative changes in the intervertebral disc. In conducting studies, special attention should be paid to the T7, T8, and T9 vertebrae, given that the lower angle of the scapula correlates with the position of these vertebrae. In addition, observation of the part of the shoulder blades is one of the most critical components of the physical examination procedure. The asymmetry of the position of these structures is a sign of spinal disorders [6]. |
|
| Image capturing is carried out to ensure statistically significant characteristics of the assessment of spinal migration. The best method and parameters for capturing an image of the patient's back using a camera may change depending on several characteristics, such as the lighting conditions, the type of camera being used, and the purpose of the image. However, here are some general guidelines that have been followed for the best results: |
|
| A lens with a broad aperture, such as f/1.8 or f/2.8, will allow lighter to enter the camera and produce a shallow depth of field, which can help to blur the background and make the subject stand out. The subject should be positioned so that their back faces the camera and their entire back is visible. Good lighting is essential for capturing a clear and well-exposed image. If shooting indoors, natural lighting or additional lighting sources such as a light source were used. A fast shutter speed will help to freeze any motion and prevent blur in the image. A good starting point would be a shutter speed of 1/125th a second. A low ISO setting will reduce digital noise in the image, resulting in a cleaner and sharper image. Start with an ISO of 100 or 200. Use the camera's auto-focus or manual focus to ensure the subject is in focus. It is crucial to focus accurately to achieve the best results. The focal length will depend on the subject's distance from the camera and the desired composition of the image. |
|
| By following these guidelines, capturing a clear and well-composed image of a person's back using a camera was done. The resulting image footage is used for further image processing and automatic estimation of the displacement of reflective measuring markers attached to the vertebrae of interest and the formation of graphs reflecting the migration of vertebrae when walking. |
|
| In the second stage of the study, frame-by–frame image reading is used, identification of the vertebral mapping cadres when the heel of the left and right feet of the subject touches the support, displacement of the point - |
|
| the conditional center of gravity of the patient's figure determines the nature of vertebral migration depending on the removal of this center. |
|
| In the third stage, an optical measuring grid is navigated and superimposed on the patient's back to accurately assess the location of the coordinates of the reflective markers and the formation of the coordinate matrix of the measuring markers for all analyzed image frames. |
|
| In the fourth stage, the calculation of diagnostically significant indicators of migration of calls during walking is carried out based on estimates of changes in the coordinates of reflective measuring markers from frame to frame and the formation of the dependence of the migration of vertebrae located in the chest, diaphragm, and lumbar spine. |
|
|
The patient is walking is recorded in the absence of any weight load on the musculoskeletal system and when burdened with a metered load utilizing a weight of a certain weight and design fixed on the patient's shoulders. The metered load on the musculoskeletal system and the spine makes it possible to simulate the nature of vertebral migration when moving in a situation where the patient is carrying heavy objects, including asymmetrically fixed ones.

|
|
| 2.An algorithm for automatic navigation of the measuring grid on the image of the patient's back to form a matrix of offset coordinates of measuring markers. |
|
| An algorithm for automatic navigation of the measuring grid on the image of the patient's back to form a matrix of offset coordinates of measuring markers. |
|
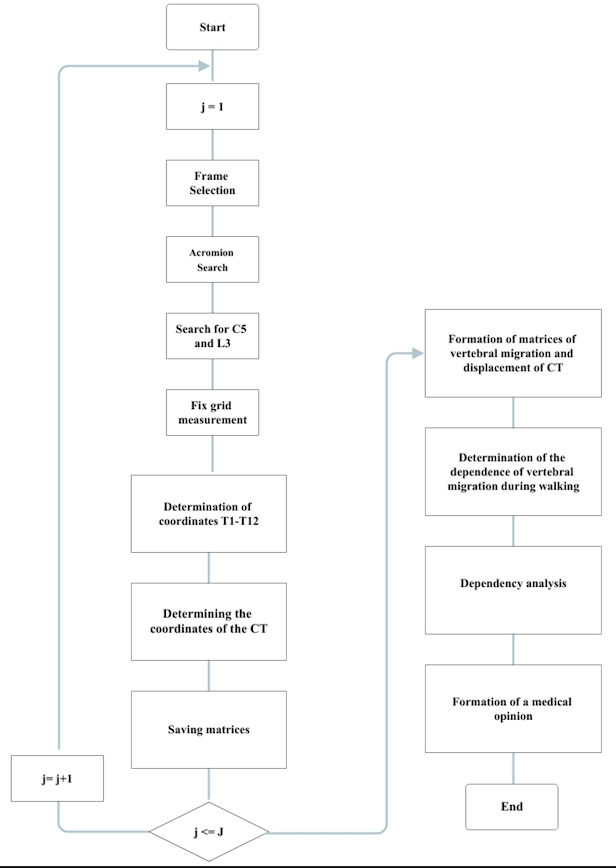
| The proposed algorithm for automatic navigation of the measuring grid consists of the following stages (Figure 1). The algorithm of intuitive navigation of the optical measuring grid begins with sampling the first frame of the image. For example, in the picture of the patient's back, two red markers located on the axillary processes of the shoulder are automatically searched for, and the measuring grid's horizontal (abscissa axis) is fixed on the identified markers. Similarly, the search for red markers on the C5 and L3 vertebrae is carried out. Next, the coordinates of the measuring markers T1–T12 and the coordinates of the conditional center of gravity of the patient are determined. |
|
| Finally, the matrices of the coordinates of the measuring markers and the center of gravity of the patient's figure are saved. This procedure is carried out for all frames J of the image capturing of the patient walking from the back. |
|
| Upon determining the markers' coordinates and the gravity center of the patient, matrices of vertebral migration and displacement of the patient's gravity center are formed from all image frames J. The functional dependence of vertebral migration on the walking phase is determined, considering the removal of the conditional center of gravity of the patient's figure. Functional dependency, a procedure, is used to approximate the frame-by-frame displacement of the coordinates of the studied vertebrae from the walking phase. |
|
 |
|
| Fig.1 The algorithm of automatic navigation of the measuring grid on the image of the patient's back with a set of support and measuring markers when walking. |
|
| The next stage of the study is an analysis of the functional dependencies of the marked vertebrae displacement from the walking phase, besides forming a medical opinion on the kinematics of the spine. |
|
| As noted above, to obtain statistically reliable results in assessing the migration of calls, image capturing is carried out within 5 or 10 minutes, because of which 300 or 600 frames of image capturing during the patient walking. Therefore, manual processing of many such images is impossible. In this regard, an algorithm for automatically navigating the measuring grid to markers fixed in the region of the acromion, C5, and L3 processes was proposed and implemented. |
|
| Therefore, when carrying out rehabilitation measures to correct spinal curvature and deformation of the intervertebral disc, it is not difficult to fix the support markers in the area of the acromion processes, C5 and L3. Furthermore, the vertebrae of interest use the proposed method and algorithm for assessing spinal kinematics disorders. Therefore, it is possible to compare the nature of vertebral migration in different patient conditions, for example, during periodic preventive examinations, at different treatment periods, without and with the use of a technical means of rehabilitation or in the process of setting it up for the patient. |
|
| The proposed algorithm was tested while developing an information and measurement system for assessing spinal kinematics disorders in the frontal plane when walking. Figures 2,3, and 4 show screenshots of the screen at various stages of the algorithm implementation. |
|
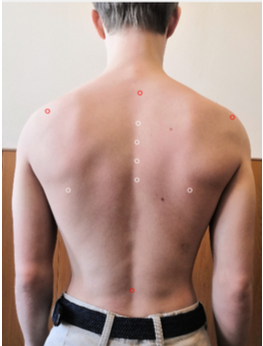
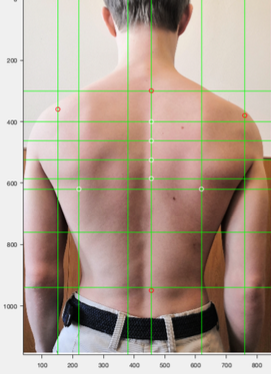
| Fig. 2 demonstrates the fixation of 4 reference markers and 6 measuring markers. Fig.3 reflects the formation of the abscissa and ordinate axes through reference markers. Fig.4 demonstrates the stage of determining the coordinates of measuring markers. |
|
 |
|
| Fig.2 image of reference and measuring markers on the back. |
|
 |
|
| Fig.3 Measuring grid lines through reference markers. |
|
.png) |
|
| Fig.4 Determination of the coordinates of measuring markers |
|
| Navigation of the measuring grid's accuracy, the navigation of the measuring grid, and the estimation of the coordinates of the measuring markers are significantly influenced by the size of the markers. Reducing the size of markers to 3-5 mm allows for an increase in the fixation accuracy substantially. However, it is necessary to use a high-resolution camera and sensitivity to identify them on an image frame. The implementation of the recommendations for selecting markers and cameras allows us to assess the migration of vertebrae when walking with an accuracy of 1 mm. |
|
|
Experimental approbation of the proposed method, including the algorithm of automatic navigation of the measuring grid, confirmed the correctness of their use to assess violations of the kinematics of the vertebral column in the frontal plane while walking.
|
|
| 3.Discussion and Conclusion |
|
| The high frequency of observation of cases of posture disorders and spinal deformities, the need for early detection of functional manifestations of these pathological conditions, and control of their dynamics during treatment necessitate the development of methods for assessing violations of the kinematics of the spine when walking. |
|
| The previous articles [7-12] reviewed different algorithms and techniques for assessing spinal deformities during walking. These techniques include optical motion capture systems, pressure-sensitive mats, inertial measurement units, and X-ray imaging. The algorithm selection depends on factors such as the research question, available equipment, and the subject population. These techniques have different levels of complexity, accuracy, and invasiveness, and researchers must carefully select the appropriate technique for their study. |
|
| The review highlights that motion capture systems are widely used for assessing spinal deformities during walking. This technique involves placing reflective markers on specific points of the body, such as the spine, pelvis, and lower limbs, and capturing their motion using multiple cameras. The data is then processed to reconstruct a 3D body model, and the spinal curvature can be measured from the model. The review also highlights pressure-sensitive mats and inertial measurement units, which offer non-invasive and portable alternatives to motion capture systems. |
|
| The previous articles [7-12] provide valuable insights into the different algorithms and techniques for assessing spinal deformities during walking. These techniques can help researchers and clinicians better understand the biomechanics of spinal deformities and develop targeted interventions to improve gait and quality of life for affected individuals. However, future research is needed to validate these techniques and further explore their clinical applications. |
|
| The proposed algorithm of assessment is based on the use of modern information technologies. It includes an image capturing of the patient's movement in projection on the frontal plane with reflective markers fixed in the spine area, automatic navigation of the optical measuring grid to the reference points of the image of the subject's body (acromion, C5, and L3 vertebrae), assessment of the migration of T1–T12 vertebrae during the frontal plane for different phases of walking. The algorithm was tested on 20 images of 5 patients during different walking times |
|
| The approximation of the coordinates of the migration of measuring markers by functions allows us to visually reproduce the nature of the kinematics of the spine in the frontal plane when walking. It is used both during screening examinations to identify functional signs of spinal deformity and for monitoring during treatment. |
|
| 4.References |
|
| |
|
| 1. Leroux M.A., Zabjek K., Simard G., etc. (2000). A Noninvasive Anthropometric Technique for Measuring Kyphosis and Lordosis. SPINE. Volume 25, Number 13, pp 1689–1694. |
|
| 2. Ubert A. I. 2021. Algorithm for markers detection on fringe images. IOP Conf. Series: Materials Science and Engineering . 012060. IOP Publishing. 2021. doi:10.1088/1757-899X/1019/1/012060. |
|
| 3. Ugwueke E. Hasan Bou Issa H. Ibrahim A.. 2022. Analytical comparison between Biomechanics parameters for normal and Crouch gait. Conference of Russian Young Researchers in Electrical and Electronic Engineering. Bioengineering System, Saint-Petersburg Electrotechnical University. |
|
| 4. Fukuchi, C.A., Fukuchi, R.K. and Duarte, M., 2019. Effects of walking speed on gait biomechanics in healthy participants: a systematic review and meta-analysis. Systematic reviews, 8(1), pp.1-11. |
|
| 5. Hasan Bou Isaa H., Ibrahim A.,Yuldashev Z., 2022, Development of a mathematical model for a moving platform for the diagnosis of the spinal state. Conference of Russian Young Researchers in Electrical and Electronic Engineering. Bioengineering System, Saint-Petersburg Electrotechnical University. |
|
| 6. Cooperstein, R., Haneline, M. and Young, M. (2015). The location of the inferior angle of the scapula in relation to the spine in the upright position: a systematic review of the literature and meta-analysis. Chiropractic & manual therapies, 23(1), pp.1-8. |
|
| 7. Nault, M.L., Allard, P., Hinse, S., Le Blanc, R., Caron, O., Labelle, H. and Sadeghi, H., (2002) . Relations between standing stability and body posture parameters in adolescent idiopathic scoliosis. Spine, 27(17), pp.1911-1917. |
|
| 8. Burwell, R.G., Clark, E.M., Dangerfield, P.H. and Moulton, A., (2016). Adolescent idiopathic scoliosis (AIS): a multifactorial cascade concept for pathogenesis and embryonic origin. Scoliosis and spinal disorders, 11(1), pp.1-7. |
|
| 9. Cook, J.B., Riccio, A.I., Anderson, T., Chen, W., Shaha, S.H. and Wimberly, R.L., (2016). Outcomes after surgical treatment of adolescent intra-articular distal humerus fractures. Journal of Pediatric Orthopaedics, 36(8), pp.773-779. |
|
| 10. Sangeux, M., (2015). On the implementation of predictive methods to locate the hip joint centres. Gait & posture, 42(3), pp.402-405. |
|
| 11. Wong, A.Y., Karppinen, J. and Samartzis, D., (2017). Low back pain in older adults: risk factors, management options and future directions. Scoliosis and spinal disorders, 12(1), pp.1-23. |
|
| 12. Chu, E.C.P., Cheng, H.Y., Huang, K., Yao, K., Zhao, J., Huang, K.H.K., Yau, K. and Zhao, J.G., (2023). Conservative management of low back pain and scoliosis in a patient with rheumatoid arthritis: eight years follow-up. Cureus, 15(3). |
|
|
|
|




